
Description
The biceps muscle is located in the front of your upper arm. It is attached to the bones of the shoulder and elbow by tendons — strong cords of fibrous tissue that attach muscles to bones.
Tears of the biceps tendon at the elbow are uncommon. They are most often caused by a sudden injury and tend to result in greater arm weakness than injuries to the biceps tendon at the shoulder.
Once torn, the biceps tendon at the elbow will not grow back to the bone and heal. Other arm muscles make it possible to bend the elbow fairly well without the biceps tendon. However, they cannot fulfill all the functions of the elbow, especially the motion of rotating the forearm from palm down to palm up. This motion is called supination.
To return arm strength to near normal levels, surgery to repair the torn tendon is usually recommended. However, nonsurgical treatment is a reasonable option for patients who may not require full arm function.
")
")
")
AnatomyHello
The biceps muscle has two tendons that attach the muscle to the shoulder and one tendon that attaches at the elbow. The tendon at the elbow is called the distal biceps tendon. It attaches to a part of the radius bone called the radial tuberosity, a small bump on the bone near your elbow joint.
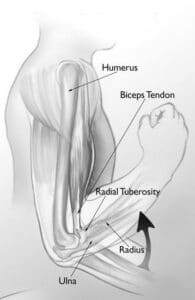
The biceps muscle helps you bend and rotate your arm. It attaches at the elbow to a small bump on the radius bone called the radial tuberosity.
Reproduced and modified from The Body Almanac © American Academy of Orthopaedic Surgeons, 2003.
CausehELLO
The main cause of a distal biceps tendon tear is a sudden injury. These tears are rarely associated with other medical conditions.
Injury
Injuries to the biceps tendon at the elbow usually occur when the elbow is forced straight against resistance. It is less common to injure this tendon when the elbow is forcibly bent against a heavy load.
Lifting a heavy box is a good example. Perhaps you grab it without realizing how much it weighs. You strain your biceps muscles and tendons trying to keep your arms bent, but the weight is too much and forces your arms straight. As you struggle, the stress on your biceps increases and the tendon tears away from the bone.
Risk Factors
Men, age 30 years or older, are most likely to tear the distal biceps tendon.
Additional risk factors for distal biceps tendon tear include:
Smoking:
Nicotine use can affect tendon strength and quality.
Corticosteroid medications:
Using corticosteroids has been linked to increased muscle and tendon weakness.
SymptomsHello
- Swelling in the front of the elbow
- Visible bruising in the elbow and forearm
- Weakness in bending of the elbow
- Weakness in twisting the forearm (supination)
- A bulge in the upper part of the arm created by the recoiled, shortened biceps muscle
- A gap in the front of the elbow created by the absence of the tendon
Doctor Examination
Physical Examination:
After discussing your symptoms and how the injury occurred, your doctor will examine your elbow. During the physical examination, your doctor will feel the front of your elbow, looking for a gap in the tendon. He or she will test the supination strength of your forearm by asking you to rotate your forearm against resistance. Your doctor will compare the supination strength to the strength of your opposite, uninjured forearm.
Imaging Tests:
In addition to the examination, your doctor may recommend imaging tests to help confirm a diagnosis.
- X-rays: Although x-rays cannot show soft tissues like the biceps tendon, they can be useful in ruling out other problems that can cause elbow pain.
- Ultrasound: This imaging technique can show the free end of the biceps tendon that has recoiled up in the arm.
- Magnetic resonance imaging (MRI): These scans create better images of soft tissues. They can show both partial and complete tears of the biceps tendon.
Treatment
Surgery to reattach the tendon to the bone is necessary to regain full arm strength and function.
Nonsurgical treatment may be considered if you are older and less active, or if the injury occurred in your nondominant arm and you can tolerate not having full arm function. Nonsurgical treatment may also be an option for people who have medical problems that put them at higher risk for complications during surgery.
Nonsurgical Options
- Rest. Avoid heavy lifting and overhead activities to relieve pain and limit swelling. Your doctor may recommend using a sling for a brief time.
- Nonsteroidal anti-inflammatory medications. Drugs like ibuprofen and naproxen reduce pain and swelling.
- Physical therapy. After the pain decreases, your doctor may recommend rehabilitation exercises to strengthen surrounding muscles in order to restore as much movement as possible.
Surgical Options
Surgery to repair the tendon should be performed during the first 2 to 3 weeks after injury. After this time, the tendon and biceps muscle begin to scar and shorten, and restoring arm function with surgery may not be possible. While other options are available for patients requesting late surgical treatment for this injury, they are more complicated and generally less successful.
Procedure: There are several different procedures to reattach the distal biceps tendon to the forearm bone. Some doctors prefer to use one incision at the front of the elbow, while others use small incisions at both the front and back of the elbow.

Figure: One method for reattaching the tendon is through a single incision at the inside of the elbow.
Reproduced from Mirzavan R, Lemos SE, Brooks K: Surgical treatment of distal biceps tendon rupture. Orthopaedic Knowledge Online Journal 2007; accessed January 2016.
A common surgical option is to attach the tendon with stitches through holes drilled in the radius bone. Another method is to attach the tendon to the bone using small metal implants (called suture anchors).
There are pros and cons to each approach. Be sure to carefully discuss the options available with your doctor.

(Left) A suture and suture anchor. (Right) This x-ray taken from the side shows where the suture anchors are placed in the radius bone.
ComplicationsH
Surgical complications are generally rare and temporary.
- Numbness and/or weakness in the forearm can occur and usually goes away.
- New bone may develop around the site where the tendon is attached to the forearm bone. While this usually causes little limitation of movement, sometimes it can reduce the ability to twist the forearm. This may require additional surgery.
- Although uncommon, the tendon may re-rupture after full healing of the repair.
RehabilitationH
Right after surgery, your arm may be immobilized in a cast or splint.
Your doctor will soon begin having you move your arm, often with the protection of a brace. He or she may prescribe physical therapy to help you regain range of motion and strength.
Resistance exercises, such as lightly contracting the biceps or using elastic bands, may be gradually added to your rehabilitation plan.
Be sure to follow your doctor’s treatment plan. Since the biceps tendon takes over 3 months to fully heal, it is important to protect the repair by restricting your activities.
Light work activities can begin soon after surgery. But heavy lifting and vigorous activity should be avoided for several months.
Although it is a slow process, your commitment to your rehabilitation plan is the most important factor in returning to all the activities you enjoy.
Surgical Outcome
Almost all patients have full range of motion and strength at the final follow-up doctor visit.
After time, return to heavy activities and jobs involving manual labor is a reasonable expectation.