
Description
Dupuytren’s disease is a condition that affects the fascia—the fibrous layer of tissue that lies underneath the skin in the palm and fingers. In patients with Dupuytren’s, the fascia thickens, then tightens over time. This causes the fingers to be pulled inward, towards the palm, resulting in what is known as a “Dupuytren’s contracture.”
In some patients, a worsening Dupuytren’s contracture can interfere with hand function, making it difficult for them to perform their daily activities. When this occurs, there are nonsurgical and surgical treatment options available to help slow the progression of the disease and improve motion in the affected fingers.

AnatomyHello
The fascia is a layer of tissue that helps to anchor and stabilize the skin on the palm side of the hand. Without the fascia, the skin on your palm would be as loose and moveable as the skin on the back of your hand. In patients with Dupuytren’s disease, this palmar fascia slowly begins to thicken, then tighten.
Often, Dupuytren’s is first detected when lumps of tissue, or nodules, form under the skin in the palm. This may be followed by pitting on the surface of the palm as the diseased tissue pulls on the overlying skin.

Figure: A Dupuytren’s contracture. The patient cannot fully extend his ring finger because of the tethering effect of the cord-like structure in his palm.
As Dupuytren’s progresses, bands of fascia in the palm develop into thick cords that can tether one or more fingers and the thumb into a bent position. This is called a “Dupuytren’s contracture.” Although the cords in the palm may look like tendons, the tendons are not involved in Dupuytren’s.
In many cases, a Dupuytren’s contracture progresses very slowly, over a period of years, and may remain mild enough such that no treatment is needed. In moderate or severe cases, however, the condition makes it difficult to straighten the involved digits. When this happens, treatment may be needed to help reduce the contracture and improve motion in the affected fingers. Typically, as a contracture worsens, the involvement of the fascia becomes more severe and treatment is less likely to result in a full correction.
CausehELLO
The cause of Dupuytren’s disease is not completely known, but most evidence points towards genetics as having the most important role.
There are anecdotal reports of Dupuytren’s emerging or worsening after a patient experiences an injury or an open wound (including surgery) to his or her hand; however, there is no good evidence to support this. There is also no compelling evidence to suggest that it is caused by overuse of the hand.
SymptomsHello
A Dupuytren’s contracture typically progresses very slowly, over a period of years. Signs and symptoms of the condition may include:
- Nodules: You may develop one or more small lumps, or nodules, in the palm of your hand. These nodules are typically fixed to the overlying skin. Initially, the nodules may feel tender but, over time, this tenderness usually goes away. In some cases, there can be “pitting” or deep indentation of the skin near the nodules.
- Cords: The nodules may thicken and contract, contributing to the formation of dense and tough cords of tissue under the skin. These cords can restrict or tether the fingers and thumb from straightening or from spreading apart.

Figure: In a Dupuytren’s contracture, nodules under the skin thicken, forming cords of tissue that pull the involved fingers inward towards the palm.
- Contractures: As the tissue under the skin tightens, one or more of your fingers may be pulled toward your palm and may be restricted from spreading apart. The ring and little fingers are most commonly affected, but any or all of the fingers can be involved, even the thumb. Most commonly, the first joint (knuckle joint) of the finger is affected, but the other joints may also be involved.
As the bend in your finger increases, it may be hard to straighten it fully. It may be difficult to grasp large objects, put your hand in your pocket, or perform other simple activities.
Some patients with Dupuytren’s disease may develop thickened tissue on the feet (Ledderhose disease) or penis (Peyronie’s disease). Symptoms do not occur anywhere else on the body.
Doctor Examination
Your doctor will talk with you about your general health and medical history and ask about your symptoms. Because Dupuytren’s can run in families, your doctor may ask if you are aware of any relatives that have the disease.
Your doctor will then carefully examine your fingers and hand. During the exam, he or she will:
- Record the location of nodules and cords on your palm.
- Measure the range of motion of your fingers and thumb.
- Test the feeling in your fingers and thumb.
- In some cases, document the appearance of your hand with clinical photographs.
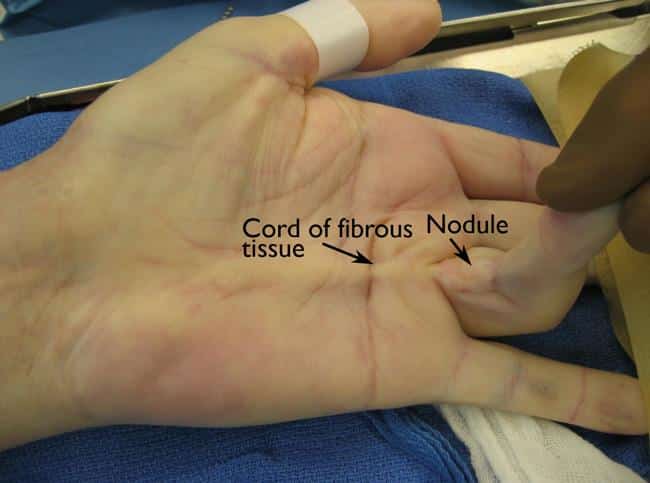
Figure: During the exam, your doctor will measure the contracture in your finger, and record the location of the cords and nodules.
These measurements will be compared with other measurements taken throughout your treatment to determine whether the condition is progressing over time.
Treatment
Currently, there is no cure for Dupuytren’s; however, the condition is not dangerous. Although it varies from patient to patient, Dupuytren’s usually progresses very slowly and may not become troublesome for many years. In fact, for some patients, the condition may never progress beyond developing lumps in the palm. If the condition progresses, your doctor may first recommend nonsurgical treatment to help slow the disease.
Nonsurgical Options
- Steroid injection: Corticosteroids are powerful anti-inflammatory medications that can be injected into a painful nodule. In some cases, a corticosteroid injection may slow the progression of a contracture. The effectiveness of a steroid injection varies from patient to patient.
- Splinting: Splinting is not known to prevent the progression of a finger contracture. Forceful stretching of the contracted finger may not be helpful and, in fact, could cause an injury to the finger or hand.
Splinting may be used after surgery for Dupuytren’s contracture to protect the surgical site; however, it is not known if it reduces the risk of recurrent contracture or tightening of the healing wound.
Recovery
Severe problems are not common after surgery, but you should expect some pain, swelling, and stiffness. Although the goal of surgery is to improve digital straightening, sometimes patients can lose flexion of the involved digits due to stiffness. Elevating your hand above your heart and gently moving your fingers will help decrease swelling and should improve stiffness.
Physical therapy can help improve strength and function in your fingers and hand, reduce swelling, and aid in wound care. Often, a hand therapist will make a splint for you to wear during recovery.

Figure: You may need to wear a splint to help protect your hand after surgery.
Outcomes
Most patients have improved movement in their fingers after surgery. However, because the condition is not “cured” with surgery, about 20 percent of patients will experience a meaningful degree of contracture recurrence. Additional surgery may be required for some patients.
Surgical Options
If the contracture interferes with hand function, your doctor may recommend surgical treatment. The goal of surgery is to reduce the contracture and improve motion in the affected fingers.
There is no known cure for Dupuytren’s contracture; however, surgery is intended to “set back the clock” by reducing the restricting effect of the cords by either disrupting or removing them. Unfortunately, the healing tissues will form with the same potential to develop cords in the future—but the gains in hand function can still be substantial.
The surgical procedures most commonly performed for Dupuytren’s contracture are:
- Fasciotomy
- Subtotal palmar fasciectomy
Your doctor will talk with you about which procedure is best in your case.
- Fasciotomy:
In this procedure, your doctor will make an incision in your palm and then divide the thickened cord(s) of tissue. Although the cord itself is not removed, dividing it helps to decrease the contracture and increase movement of the affected finger.
Fasciotomy is performed using a local anesthetic that numbs just your hand without putting you to sleep. After the procedure, your wound will be left open and allowed to heal gradually. You will have to wear a splint during your recovery.
Figure : (Left) Clinical photo shows the contracture of a patient’s little finger before fasciotomy. (Right) After the procedure, the patient is able to straighten his finger. The wound is left open to heal. -
Subtotal palmar fasciectomy:
In this procedure, your doctor will make an incision, then remove as much of the abnormal tissue and cord(s) as possible in order to straighten your finger(s). Several types of incisions can be used in a fasciectomy but, often, a “zig-zag” incision is made along the natural creases in the hand.In some cases, your wound will be left open to heal gradually on its own after fasciectomy. In other cases, a skin graft will be needed to help the wound heal. For the skin graft, your doctor will take healthy skin from another area of your body and use it to seal the wound. You may have to wear a splint during your recovery.
Subtotal palmar fasciectomy is a more extensive procedure than fasciotomy. It generally entails more wound care and physical therapy, a longer healing time, and greater patient effort during recovery.

Figure: (Left) Clinical photo shows the zig-zag incisions commonly used in a subtotal palmar fasciectomy. (Right) Following wound healing, this patient has good finger extension and improved function in his hand. - Complications:
As with any surgery, there are risks associated with surgery for Dupuytren’s contracture. The likelihood of complications increases with the following:
- The severity of the contracture
- The number of contractures addressed in a single procedure
- The presence of any other medical conditions
Your doctor will discuss each of the risks with you and will take specific measures to help avoid potential complications. Possible risks and complications of surgery for Dupuytren’s include:
- Pain
- Scarring
- Injury to nerves and/or blood vessels
- Wound infection
- Stiffness
- Loss of sensation. Temporary loss of sensation may result from stretching nerves that have been contracted for a long time.
- Loss of viability of a finger/loss of a finger (rare)
Recent Developments in Treatment
The recently developed treatments described below are intended to reduce a contracture and improve motion in the affected fingers by disrupting the tethering effect of the Dupuytren’s cords.
Enzyme InjectionH
The injection of an enzyme solution for treatment of Dupuytren’s contracture has recently been approved by the Federal Drug Administration. The enzyme, a collagenase, is administered on an outpatient basis by doctors who have been specifically trained in the technique.
To begin, your doctor will inject the enzyme directly into the cords in your hand. During the 24 to 72 hours following the injection, the enzyme will weaken/dissolve the contracted tissue.
The next step is performed under local anesthesia. Your doctor will manipulate and straighten your bent fingers to break or pull apart the restrictive cords. Often, this improves the contracture and increases range of motion in the fingers.
Enzyme injection typically results in less pain and swelling than major surgery. Although rare, the injection may cause an allergic reaction or flexor tendon rupture. Other potential complications are the same as those for surgery.
Early results for enzyme injection are promising, but long-term results and recurrence rates are not yet known.
Needle Aponeurotomyh
This relatively new, minimally invasive procedure is performed on an outpatient basis by doctors specifically trained in the technique.
During the procedure, your doctor will first numb your hand with a local anesthetic. He or she will then pass the sharp end of a hypodermic needle back and forth through the restrictive cords to weaken and rupture the diseased tissue. The diseased tissue is not removed but, rather, is lengthened by breaking it apart.
The complications of needle aponeurotomy are similar to those of surgery, as far as recurrence, nerve or blood vessel injury, pain, and stiffness.
Early results for needle aponeurotomy appear similar to those of surgery and enzyme injection, but long-term recurrence rates are not yet known.